INTRODUCTION
Polyethylene glycol (PEG) is a chemically inert, amphiphilic polymer used as an excipient in many pharmaceuticals for decades, and as a conjugate with biologicals (ie, PEGylation) since 1990. To date, the US FDA has approved 14 PEGylated therapies with diverse indications. Although it is recognized that such products contain PEG, there may be a lack of awareness regarding the use of large quantities of excipient PEG in factor VIII (FVIII) and factor IX (FIX) therapies for hemophilia A and B, respectively, as well as in other parenteral therapies administered long term in the pediatric population. Due to concern about the potential toxicity of long-term exposure to PEG, particularly in children, based primarily on preclinical observations of cellular vacuolation upon supratherapeutic dosing of PEG molecules ≥ 40kDa (EMA. Safety Working Party's Response to the PDCO Regarding the Use of PEGylated Drug Products in the Pediatric Population; 2012. ), we evaluated the total PEG content of these therapies. Our objective was to estimate annual PEG exposure from each product as commonly prescribed, and to determine whether any adverse events (AEs) reported could be attributed specifically to PEG.
METHODS
FDA-approved parenteral therapies with pediatric indications were analyzed for PEG exposure per dose and per year. For comparative purposes, we grouped FVIII products together as primary comparators to Antihemophilic Factor (Recombinant), PEGylated (ADYNOVATE®).
To quantify excipient PEG, we included free PEG of various molecular weight and excipients with chemical structures containing PEG chains (polysorbate 20 [PS20] and 80 [PS80], and poloxamer 188 [P188]). For FVIII and FIX therapies, PEG exposure was calculated based on a range of dosages recommended in the 2013 World Federation of Hemophilia Guidelines (25-40 IU/kg; Srivastava, et al. Haemophilia . 2013; 19:e1-e47). For extended half-life recombinant (r)FVIII and rFIX products and all other products, exposure was calculated based on prescribing information (PI), including a given dosage range. Three weights were used to cover the pediatric population: 10, 30, and 50 kg, with exceptions pertaining to the PI. The formula used to calculate PEG exposure per dose was:
PEGylated biologic: patient weight (kg) × dose (IU or mg/kg) × (PEG MW/total MW)/specific activity
Excipient PEG: patient weight (kg) × dose ((IU or mg)/kg)/(PEG concentration) × PEG ratio *
*Ratio: PEG/PEG=1; for PS80, PEG/PS80=0.645; for P188, PEG/P188=0.69.
For this analysis, combinations of vial sizes were pragmatically chosen to minimize factor waste, leading to some variability in dosing. All PEG molecules were treated equally, whether conjugated or present as an excipient and regardless of size or structure.
Safety outcomes were investigated by searching the medical literature for any report of clinical PEG-related AEs, and by attempting to identify any salient pattern of AEs listed in the PI or reported to the FDA or other reporting organization that might reflect PEG toxicity.
RESULTS
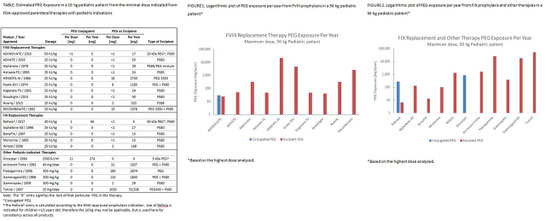
For a child weighing 10 kg and receiving minimal prophylaxis dosages of FVIII, total PEG exposure ranged from <1 to 2,730 mg/year; for prophylaxis with FIX products the range was <1-168 mg/year. For other products, total PEG exposure ranged from 2 to 53,508 mg/year (Table 1). For a child weighing 50 kg and receiving maximum prophylaxis dosages of FVIII, total PEG exposure ranged from 40 to 21,840 mg/year; for prophylaxis with FIX products, the range was 13-1,342 mg/year. For other products, total PEG exposure ranged from 383 to 53,508 mg/year (Figure 1 and 2). Eloctate®, which contains PEG in the form of excipient PS20, had insufficient publicly available information to determine PEG exposure. There were no reports in the medical literature of clinical safety issues or signals specifically attributed to long-term exposure to PEG; and no recognizable patterns or trends of central nervous system, hepatic, allergic, or renal AEs.
CONCLUSIONS
Pediatric exposure to PEG from FVIII, FIX, and other parenteral therapies has occurred for decades. Exposure to PEG as an excipient has been greater than exposure to PEG as a component of a PEGylated therapy. Notably, exposure to PEG from ADYNOVATE, including excipient and conjugated forms, is comparable to or less than that from other FVIII products. There were no discoverable reports of toxicity attributed to PEG accumulation from use of these products.