The increasing number of poorly water-soluble drug candidates in pharmaceutical development is a major challenge. Enabling techniques such as amorphization of the crystalline drug can result in supersaturation with respect to the thermodynamically most stable form of the drug, thereby possibly increasing its bioavailability after oral administration. The ease with which such crystalline drugs can be amorphized is known as their glass forming ability (GFA) and is commonly described by the critical cooling rate. In this study, the supersaturation potential, i.e., the maximum apparent degree of supersaturation, of poor and good glass formers is investigated in the absence or presence of either hypromellose acetate succinate L-grade (HPMCAS-L) or vinylpyrrolidine-vinyl
acetate copolymer (PVPVA64) in fasted state simulated intestinal fluid (FaSSIF). The GFA of cinnarizine, itraconazole, ketoconazole, naproxen, phenytoin, and probenecid was determined by
melt quenching the crystalline drugs to determine their respective critical cooling rate. The inherent
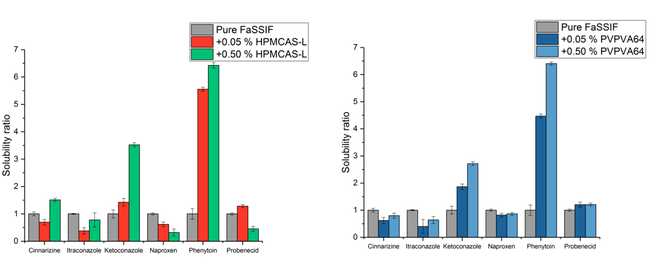
supersaturation potential of the drugs in FaSSIF was determined by a solvent shift method where the respective drugs were dissolved in dimethyl sulfoxide and then added to FaSSIF. This study showed that the poor glass formers naproxen, phenytoin, and probenecid could not supersaturate on their own, however for some drug:polymer combinations of naproxen and phenytoin, supersaturation of the drug was enabled by the polymer. In contrast, all of the good glass formers—cinnarizine, itraconazole, and ketoconazole—could supersaturate on their own. Furthermore, the maximum achievable concentration of the good glass formers was unaffected by the presence of a polymer.