The story of how we came to use inhaled mannitol to diagnose asthma and to treat cystic fibrosis began when we were looking for a surrogate for exercise as a stimulus to identify asthma. We had
proposed that exercise-induced asthma was caused by an increase in osmolarity of the periciliary fluid. We found hypertonic saline to be a surrogate for exercise but an ultrasonic nebuliser was
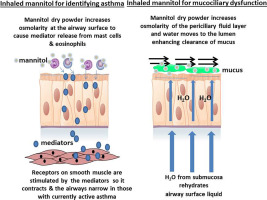
required. We produced a dry powder of sodium chloride but it proved unstable. We developed a spray dried preparation of mannitol and found that bronchial responsiveness to inhaling mannitol
identified people with currently active asthma. We reasoned that mannitol had potential to replace the ‘osmotic’ benefits of exercise and could be used as a treatment to enhance mucociliary clearance
in patients with cystic fibrosis. These discoveries were the start of a journey to develop several registered products that are in clinical use globally today.